The world's most powerful antidepressant is already in a billion lungs
MAO inhibitors are massively underutilized by psychiatrists and biohackers. Reversing age-related increases in MAO levels could restore youthful cognition and drive.
2025-09-30
I love drugs psychopharmacology.
Psychopharmacology is a fascinating subject and highly relevant to improving your life given how much of your well-being is downstream of the milieu of neurotransmitters in your brain.
There is an enzyme called monoamine oxidase (MAO) that breaks down various neurotransmitters (dopamine, serotonin, etc.).
Our MAO levels are altered more often than you might expect, for example:
- MAO levels steadily increase as you age, with a sharp increase around age 50-60
- chronic tobacco smokers have ~40% reduced MAO
- women going through perimenopause have ~30% elevated MAO
- acute stress lowers MAO activity, chronic stress massively increases it
- unmedicated depressed patients have 34% higher brain MAO, ~2 SD above the healthy mean
Monoamine oxidase inhibitors (MAOIs) are drugs that inhibit this enzyme, thus increasing the levels of various neurotransmitters.
If I were to plot all the psychoactive substances by their cultural visibility versus their potential benefit, I would place MAOIs in the far corner of esoteric and useful. Despite compelling evidence for their efficacy, they remain underutilized by psychiatrists for mood disorders and by biohackers for productivity, creativity, and longevity. Given the rising interest in biohacking, especially with the rise in productivity-maxing "grindset" culture, I'm surprised more people aren't discussing this class of drugs.
I'm going to reference studies in this, but you should probably know that I specifically looked for those studies to prove my point, so... they're really just for aesthetics. This is not intended to be a balanced comprehensive look at the pros and cons of MAOIs. I'm building a monument of confirmation bias in an attempt to avenge the reputation of a class of drugs I feel have been unjustly forgotten.
The First Antidepressant
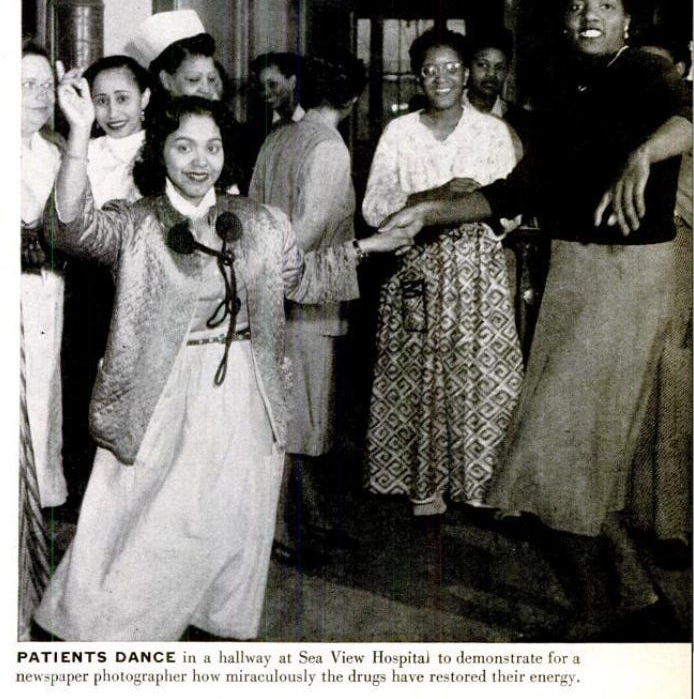
An MAOI (Iproniazid) was actually the first modern antidepressant ever created. It was intended as a tuberculosis treatment and when it was tested on patients at Sea View Hospital, it did nothing for their tuberculosis, but they did become more energetic, sociable, and optimistic--with some reports describing patients as "dancing in the halls" and "inappropriately happy".
Researchers later discovered that iproniazid worked by inhibiting MAO. Several more MAOIs quickly entered the market and were widely prescribed for depression and anxiety.
Types of MAOIs
MAOIs can be either reversible or irreversible:
- Reversible MAOIs temporarily compete with other MAO-metabolized molecules for a binding site on the MAO enzyme.
- Irreversible MAOIs form a permanent covalent bond with MAO enzymes, completely inactivating them until new enzymes are synthesized. MAO regeneration takes approximately two weeks.
MAOIs can also be selective for a specific subtype of MAO:
- MAO-A preferentially metabolizes serotonin, norepinephrine, etc.
- MAO-B preferentially metabolizes phenethylamine (an endogenous stimulant), etc.
- Both subtypes metabolize dopamine
Delayed Effect
These neurotransmitters and trace amines are elevated immediately upon taking an MAOI but patients frequently report that the drug doesn't start working properly until 1-3 months of chronic use. Some patients report that the drug continues to increase in effectiveness over the course of an entire year.
The reason is that the brain has powerful homeostatic mechanisms that keep this rise in neurotransmitters in check while the brain adapts to its new chemical environment.
The autoreceptors (basically things that check for the presence of too many neurotransmitters) need time to downregulate, and the second-order effects (synaptogenesis, hippocampal neurogenesis, etc.) need time to materialize.
The Decline of MAOIs
Unfortunately, the MAO enzyme is also responsible for breaking down dietary tyramine. People taking irreversible MAOIs must avoid foods high in tyramine (aged cheese, aged meat, etc.), otherwise the tyramine could enter the bloodstream in sufficient amounts to trigger a hypertensive crisis.
Those taking an MAOI must also avoid any drugs that significantly raise serotonin levels (SSRIs, MDMA, etc.) which could cause serotonin syndrome.
As a result of the drug-drug and food-drug interactions, MAOIs have fallen out of favor over the years.
This decline accelerated when the patents expired and pharmaceutical companies aggressively pushed their new on-patent SSRIs.
A Small but Loyal Fanbase
"MAOIs are very effective, moderately dangerous, and super hard to get". Scott Alexander has mentioned MAOIs quite a bit throughout SlateStarCodex, for example in this post about the FTX crash (because Sam Bankman-Fried was using an MAOI at the time). In this post, he aggregates patient reviews of medications and finds that two non-selective irreversible MAOIs are the highest rated drugs, and a MAO-B selective MAOI holds the number 4 spot. "This doesn’t surprise me at all. Everyone secretly knows Nardil and Parnate (the two commonly-used drugs in the MAOI class) are excellent antidepressants. Oh, nobody will prescribe them, because of the dynamic discussed here, but in their hearts they know it’s true."
MAOIs these days are only given to people who have failed every other antidepressant available--who are often forced to scrape the bottom of the treatment barrel with extreme gambles like ECT before most doctors will even consider prescribing one. So you'd expect these cases of extremely treatment-resistant depression to withstand yet another psychiatric intervention. And yet, MAOIs work often enough to top the leaderboard against first-line SSRIs often given to people whose depression would have resolved in a few months with a placebo pill.
Fans of MAOIs frequently mention:
- powerful antidepressant and axiolytic effects
- increased motivation, libido, and responsiveness to rewards
- increased emotional responsiveness and social bonding
- cognitive enhancement
There is a tiny and shrinking group of patients advocating for this class of drugs, but they advocate very hard.
Tobacco
Ironically, while the number of conscious users of pharmaceutical MAOIs is minuscule, the number of unconscious users of hidden MAOIs is massive.
Tobacco is the third most popular drug, used by over a billion people, and tobacco smoke contains numerous MAOIs.
Long-term smokers show ~30% inhibition of MAO-A and ~40% inhibition of MAO-B on average (but potentially much higher: max of n=13 was 77%). Smokers have chronically and significantly reduced MAO levels regardless of how recent the last cigarette was, suggesting that MAO is inhibited irreversibly.
Given MAO's effect on dopamine, Smokers with ADHD might be self-medicating.
Gwern has a famous nicotine essay that inspired a new cohort of nicotine addicts in Silicon Valley. Except, as Gwern points out, nicotine isn't addictive on its own. It's the synergistic effect of combining nicotine and MAOIs that makes tobacco so addictive.
As in all addictions, dopamine (DA) is ultimately the culprit. MAOIs increase DA through the suppression of DA metabolism and the stimulation of exocytotic DA production.
DA-mediated reward sensitization arises after around 1-3 months of chronic MAO inhibition. This paper found the culprit behind the delayed sensitization to nicotine: the 5-HT1a autoreceptors which take a few weeks of chronic MAOI use to downregulate.
In my personal experiments, nicotine sensitization wasn't as powerful as Factorio sensitization--bringing Factorio from a fun normal game to an all-consuming career-threatening time vortex preventing all eating and sleeping while the factory grew rapaciously until it consumed everything including its architect.
The Era of Progress
There was an accidental global experiment with MAO inhibitors that nobody talks about. Tobacco use in the first-world during the 20th century was so widespread that these MAOIs definitely quietly shaped mood, cognition, and--by extension--progress.
One could argue that the rate of human progress has been proportional to the prevalence of tobacco smoking--with the peak of both being the 1940s to 1960s.
In keeping with the spirit of this essay, I will ignore all the obvious confounders and speculate wildly: the synergy between nicotine and MAOIs unwittingly fueled humanity's golden age of innovation. These hidden MAOIs enhanced goal-directed behavior and since these smokers didn't have Factorio to get addicted to, they just built real factories instead.
The greatest engineers, scientists, and mathematicians of the age were all very heavy tobacco users (Einstein, von Neumann, Oppenheimer, Bohr, Hubble, Edison, etc.), and the great writers often credited tobacco with creativity.
Tobacco consumption began declining rapidly in the 1970s, which coincides curiously well with the timeline of the Great Stagnation. What happened in 1971? We stopped amplifying dopamine signaling.
"We wanted flying cars, instead we got 140 characters". Well then you should've kept smoking.
The Enzyme That Ages You
MAO-B in the brain increases as you age (7% per decade across the whole brain, 18% per decade in the prefrontal cortex) and this accelerates after age 50-60.
The subsequent decline in dopamine could partially explain common age-related changes:
- reduced openness to experience (less DA means less novelty-seeking)
- cognitive inflexibility (prefrontal cortext DA is crucial for set-shifting)
- reduced motivation and libido
- bradykinesia (motor slowing)
MAO-B also produces hydrogen peroxide which creates oxidative stress and neuroinflammation. Oxidative damage to dopaminergic neuron could accelerate the decline in DA, which is why MAO-B inhibitors are studied for Parkinson's disease (and why chronic smokers have a much lower rate of Parkinson's).
MAO inhibitors:
- are neurostimulative, neuroprotective, neuroregenerative, and anti-inflammatory
- improve memory in Alzheimers
- delay age-related cognitive decline in mice
- protected dopaminergic neurons from age-related decay
- restore full scale sexual activity in elderly rats
- extended lifespan by an average of 35% (this was actually the first study ever to extend lifespan of rats beyond their estimated max age of 182 weeks)
- enhance cognitive function
- reverse cellular aging (via a drug cocktail that includes the MAOI tranylcypromine)
One case report described an elderly man with treatment-resistant depression and near-dementia-level cognitive impairment who was put on an MAOI. He saw no improvements for the first few weeks. Then after 6 weeks: "substantial improvement with complete resolution of cognitive impairment". "He was noted to be quite alert and active and cheerful. His cognitive functioning seemed to have returned to normal with a score of 28 out of 30 on the Mini-Mental status examination."
I vote that we give MAOIs to all the really old people in positions of power and usher in a golden age as they all regain their youthful vitality.
The age-related reduction of DA might have been selected for by the post-reproductive "stepping aside" evolutionary pressure. But I didn't consent to stepping aside. If this enzyme really does steal our youth, then we have the science-given right to inhibit it back.
Low-hanging Fruit
So if MAO-B increases with age, why is there virtually no research on counteracting it? We could be using very low-doses of MAO-B inhibitors, just enough to restore 20-year-old MAO levels. Testosterone Replacement Therapy is widely utilized by aging men to restore youthful testosterone levels. Where is the MAO-B Reduction Therapy?
Women going through perimenopause have elevated levels of MAO-A which contributes to the depression/anxiety that many women experience during this phase. We already use Hormone Replacement Therapy to restore estrogen levels during menopause. Why has no one invented MAO-A Reduction Therapy?
There is so much low-hanging fruit surrounding MAOIs. If I were in charge of Big Pharma, this would be my strategy:
1) Address the diet restriction
Tyramine is obviously what's holding back MAOIs. No one wants to have a hypertensive crisis because they accidentally ate the wrong meal.
Bring awareness to the fact that MAO-A in the gut must be significantly inhibited (>70%) for the diet to apply. Strictly MAO-B selective inhibitors are ok--you can do age-related MAO-B Reduction Therapy without worry.
Create a MAO-A EpiPen. Accidentally ate a bunch of tyramine? No worries, just stab yourself with this needle and these little MAO-A molecules will take care of that for you.
Work on bypassing intestinal MAO-A. There is a transdermal selegiline patch (Emsam) which bypasses first-pass metabolism and as a result doesn't have any dietary restrictions. The manufacturers chickened out and added the diet requirement to high-doses (because selegiline loses selectivity), but there has never been a reported hypertensive crisis with Emsam at any dosage. However, selegiline is far less effective for mood disorders than other MAOIs. So let's create a transdermal tranylcypromine (TCP) patch.
Research the NRI+MAOI combination. Norepinephrine Reuptake Inhibitors (NRIs) prevent the tyramine pressor response (in fact, this is how scientists check if a new drug is an NRI). Many depression patients already combine an MAOI with an NRI (e.g. nortriptyline). We should run experiments on TCP+desipramine (the most selective NRI, AFAIK) and find the lowest possible dose that robustly prevents the tyramine pressor response.
Research the combination of a reversible inhibitor of MAO-A (RIMA) with an irreversible inhibitor of MAO-B (e.g. moclobemide+selegiline). The reversibility of the MAO-A inhibition would remove the dietary restriction.
Then patent the MaoEpiPen, the transdermal TCP, the NRI/MAOI mixture, and the RIMA mixture. Now you can make money from MAOIs again.
2) Conduct better studies
Run longer studies. So many MAOI studies are far too short. It takes a long time for the benefits of MAOIs to fully materialize.
Experiment with lower doses.
- The minimal dose of every current irreversible MAOI is way too high--the lowest-dose will nearly fully inhibit MAO after a couple weeks.
- Many cognition/longevity studies show an inverted U-shaped dose-response curve. It's very important to get the dose right.
- In my personal experiments, adjusting to MAOIs by starting with very low doses (cutting up pills, waiting days between doses) results in a much better outcome.
- Some people might want a more modest inhibition like the~40% MAO inhibition of tobacco.
3) Find the right market
Beyond the obvious market of people with mood disorders, there are:
- ADHD
- perimenopause
- ex-smokers who aren't satisfied with just pure nicotine
- social anxiety
- the longevity/anti-aging crowd
- the nootropics crowd
I suspect that a nicotine+MAOI non-carcinogenic approximation of tobacco would be quite popular.
And it's also important to educate the psychiatrists. Dr. Ken Gillman is already leading the charge.
Conclusion
Hopefully this cherry-picked essay has convinced you that MAOIs deserve to be acknowledged.
Mental health disorders are skyrocketing. The population is aging. We cannot afford to ignore a class of drugs that could restore the neurochemical vigor of youth and reignite the spark of human progress.